
Ultrasound in the Initial Evaluation of Paediatric IBD
Timely and accurate assessment of intestinal inflammation at diagnosis is critical in paediatric inflammatory bowel disease (IBD). While ileo-colonoscopy is the diagnostic gold standard, it is invasive, resource‑intensive, and burdensome for children. There is a growing need for reliable, non‑invasive tools that reflect objective disease activity and support early decision‑making.
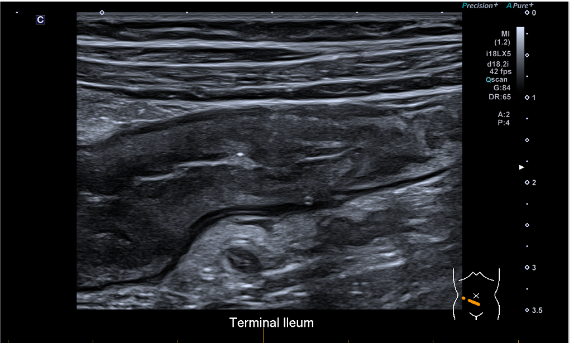
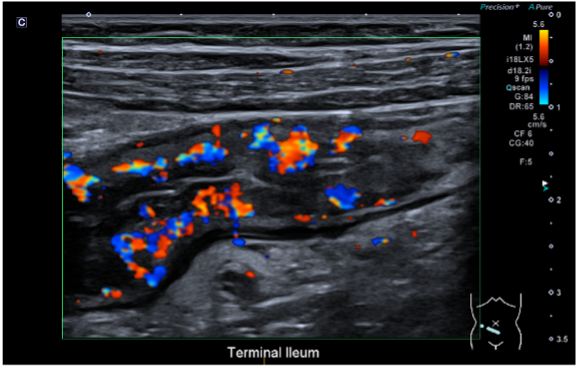
A prospective, single‑centre study evaluated intestinal ultrasound (IU) in children undergoing ileo-colonoscopy for suspected IBD. IU was performed within one month of endoscopy, with radiologists and endoscopists blinded to each other’s findings. Outcomes were compared with endoscopic severity, faecal calprotectin, and clinical disease activity indices.
Key findings
- IU demonstrated good overall diagnostic accuracy for paediatric IBD.
- Performance was strongest in moderate‑to‑severe disease, with sensitivity >90% and high negative predictive value.
- IU findings correlated closely with objective inflammatory measures, including faecal calprotectin and endoscopic severity scores.
- Correlation with symptom‑based clinical indices was poor, highlighting the limitations of relying on symptoms alone to assess inflammatory burden.
Clinical Significance
- IU reliably identifies clinically significant intestinal inflammation, particularly when disease is moderate or severe.
- Strong alignment with biomarkers and endoscopy supports IU as a valid indicator of true inflammatory activity.
- Poor correlation with clinical indices reinforces the need for objective assessment tools in paediatric IBD.
Implications for Health Services
- Diagnostic Pathways: IU can function as an early screening and risk‑stratification tool in children evaluated for IBD.
- Complementary Role: IU does not replace endoscopy but can complement biomarkers and imaging, particularly at diagnosis.
- Patient Experience: IU is non‑invasive, radiation‑free, repeatable, and well-tolerated—well-suited to paediatric care.
- Resource Optimisation: Strategic integration of IU may reduce reliance on immediate invasive procedures in selected cases and support longitudinal monitoring.
Limitations
- IU cannot provide histologic confirmation.
- Diagnostic accuracy is operator‑dependent and requires appropriate training.
- Evidence is based on single‑centre data.
Bottom Line
Intestinal ultrasound is a clinically valuable, non‑invasive modality for the initial evaluation of paediatric IBD. Its high accuracy for moderate‑to‑severe disease and strong correlation with objective inflammatory markers support its integration into paediatric IBD diagnostic pathways as a complementary tool alongside endoscopy.